Aminoglycoside Dosing
Once Daily Dosing (ODD)
Should be used in most clinical situations.
Exceptions when to consider multiple daily dosing:
- Renal impairment (CrCl < 20ml/min)
- Synergy in gram positive endocarditis
- Pregnancy
- Significant ascites
- Burns affecting > 20% BSA
- Septic shock
1. Determine patient’s dosing weight
Use ideal body weight (IBW) unless total body weight (TBW) is less, then use TBW
Use adjusted body weight (ABW) in obesity (e.g. TBW >30% over IBW)
2. Estimate creatinine clearance
CrCl (mL/min) = [(140 –age) x weight x 1.2] / sCr
* Females: x 0.85
Using Ideal Body Weight (IBW) or Adjusted Body Weight (ABW) if patient is obese (i.e. TBW > 30% over IBW)
IBW (male) = 50kg + 2.3kg (each inch > 5 ft)
IBW (female) = 45.5kg + 2.3kg (each inch > 5 ft)
Adjusted Body Weight (ABW) = IBW + 0.4 (TBW -IBW)
3. Select dose and frequency
Consult pharmacist to optimize dosing
| CrCl (mL/min) | Tobramycin / Gentamicin dose (round to nearest 20mg) | Amikacin dose (round to nearest 50mg) |
| > 60 | 5 – 7mg/kg IV q24h | 15mg/kg IV q24h |
| 40 – 59 | 5 – 7mg/kg IV q36h | 15mg/kg IV q36h |
| 20 – 39 | 5 – 7mg/kg IV q48h | 15mg/kg IV q48h |
| < 20 | use multiple daily dosing | Use multiple daily dosing |
4. Monitoring
Nephrotoxicity
- Nephrotoxicity associated with elevated trough levels, is usually reversible.
Serum creatinine to be checked at least twice weekly and levels at least once weekly or more frequent with renal function changes
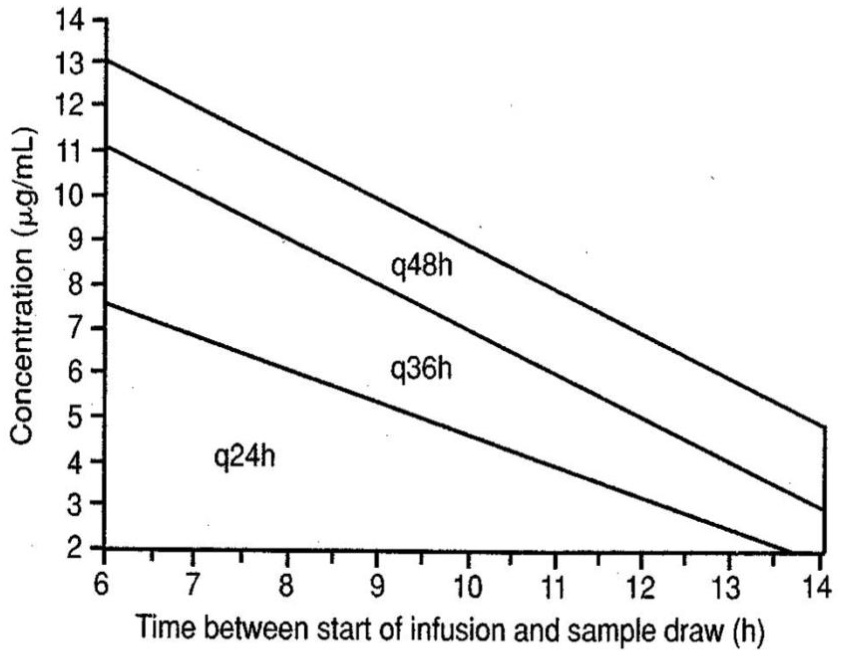
- Use the Hartford nomogram below:
- Check a random level 6-14 hours after start of st dose (please note for Amikacin: divide levels in half and then plot on graph). Tobramycin and gentamicin based on a dose of 7mg/kg, if using a dose of 5mg/kg, adjust accordingly.
- Plot level and time on graph. The point may fall into one of these 5 areas:
- Below Nomogram (< 2mg/L): Give dose q 24hrs
- Q24h, q36h, or q48h: Give dose at indicated interval
- Above Nomogram: Discontinue ODD and switch to MDD if an aminoglycoside is still warranted
- Alternatively, obtain a trough level within 30 minutes before SECOND DOSE trough should be < 1mg/L for gentamicin / tobramycin and < 4mg/L for amikacin. If level greater than indicated, contact pharmacist to assist with dosing.
Hartford Nomogram
* For multidrug resistant organisms requiring aminoglycoside therapy, please consult ID/ASP pharmacist.
Ototoxicity
Aminoglycosides may adversely affect cochlear and/or vestibular function. Ototoxicity can occur with normal drug levels and often is not reversible. Consider daily assessment of hearing and balance in patients who are alert. Consider hearing test if on prolonged therapy.
Neuromuscular Blockade
- Rare and self-limiting
- Contraindicated in myasthenia gravis
Multiple Daily Dosing (MDD)
1. Determine patient’s dosing weight
As above
2. Estimate creatinine clearance
Using equation above
3. Select dose and frequency
| CrCl (mL/min) | Tobramycin / gentamicin dose (round to nearest 20mg) | Amikacin dose (round to nearest 25mg) |
| > 60 | 2mg/kg IV q8h | 7.5mg/kg IV q12h |
| 40 – 59 | 2mg/kg IV q12h | 7.5mg/kg IV q12h |
| 20 – 39 | 2mg/kg IV q24h | 7.5mg/kg IV q24h |
| < 20 | 2mg/kg loading dose then by level | 7.5mg/kg IV x 1 then dose by level |
| HD | 2mg/kg then 1mg/kg post HD | 7.5mg/kg IV post HD |
| PD | 1.5-2mg/kg IV q48h | 7.5mg/kg IV q48h |
| CRRT | 2mg/kg IV q24-48h | 7.5mg/kg IV q24-48h |
4. Monitoring
- Serum creatinine at least twice weekly while on therapy (please always reassess need for aminoglycosides if there is a significant decline in renal function)
- Trough level just prior to THIRD DOSE; peak level 30 minutes after completion of THIRD DOSE
| Peak (mg/L) | Trough (mg/L) | |
| Gentamicin | 4 – 10 | < 2 |
| Tobramycin | 4 – 10 | < 2 |
| Amikacin | 15 – 30 | < 8 |
* peaks are general guides and are often dependent on causative organism and type of infection
When gentamicin is used in the setting of endocarditis for synergy with a beta-lactam or vancomycin against gram positive organisms (e.g. Enterococcus, Staphylococcus, Streptococcus):
Dose is 1 mg/kg at interval determined by CrCl
(see MDD dosing table)
Desired target peaks should be 3-5mg/L with trough < 1mg/L